Cangrelor in Patients With Coronary Artery Disease Pretreated With Ticagrelor: The Switching Antiplatelet
Abstract
Background
There are no studies specifically designed to rule out a drug-drug interaction (DDI) when cangrelor is used among patients who have been pretreated with ticagrelor.
Objectives
This study sought to rule out a DDI among cangrelor-treated patients who have been pretreated with ticagrelor.
Methods
In this prospective, randomized, double-blind, placebo-controlled, crossover, pharmacokinetic (PK) and pharmacodynamic (PD) study, patients with coronary artery disease (N = 20) were pretreated with a 180-mg ticagrelor loading dose and after 1 hour randomized to placebo or cangrelor (bolus and infusion for 2 hours). Patients crossed over after 1 to 4 weeks of washout. PK analysis included ticagrelor plasma levels and its active metabolite. PD assessments included VerifyNow P2Y12 reaction units (PRU), light transmittance aggregometry, vasodilator-stimulated phosphoprotein, and Total Thrombus-Formation Analysis System. PK/PD assessments were performed at 7 time points.
Results
Compared with placebo, adding cangrelor to patients pretreated with ticagrelor resulted in a significant reduction in PRU at 30 minutes and 1 hour after starting infusion. At 2 hours after stopping cangrelor/placebo infusion, PRU were low and similar in both groups (16.9 vs 12.6; mean difference: 4.3; 95% CI: −28.6 to 37.3), meeting the noninferiority primary endpoint (predefined noninferiority margin 45 PRU). Consistent findings were shown with all PD assays. PK tracked PD findings with no differences between groups in plasma levels of ticagrelor and its metabolite.
Conclusions
Compared with placebo, the use of cangrelor in patients pretreated with ticagrelor results in enhanced platelet inhibition with no differences in PK/PD profiles after discontinuation of drug infusion indicating the absence of a DDI. (PD and PK Profiles of Switching Between Cangrelor and Ticagrelor Following Ticagrelor Pre-treatment [SWAP-5]; NCT04634162)
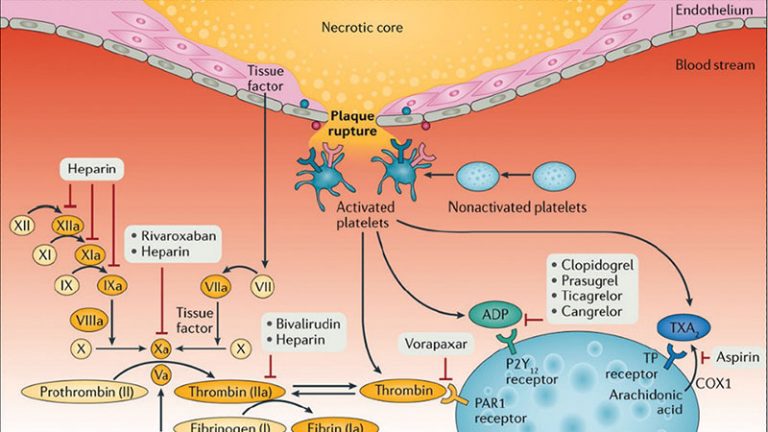
Cangrelor is an intravenous P2Y12 receptor inhibitor approved for the reduction of thrombotic events in patients undergoing percutaneous coronary intervention (PCI) who have not been pretreated with an oral P2Y12 inhibitor.1, 2, 3, 4 Given the different pharmacological properties of cangrelor and oral P2Y12 inhibitors, drug-drug interaction (DDI) may potentially occur with their concomitant administration.5,6 Importantly, a DDI may result in reduced platelet inhibition, thus mitigating the protection from thrombotic complications in the peri-PCI period.5,6 In fact, platelet P2Y12 receptors are largely occupied by cangrelor during its infusion, impeding further binding with oral agents. Because the active metabolites of thienopyridines (clopidogrel and prasugrel) have half-lives that do not exceed the duration of the recommended infusion of cangrelor (ie, 2-4 hours), they are mostly cleared from systemic circulation by the time the P2Y12 receptors become available for binding following discontinuation of cangrelor infusion.7, 8, 9, 10 Accordingly, clopidogrel and prasugrel should be administered at the end of the cangrelor infusion to avoid a DDI.5,6 Ticagrelor has a half-life of 6 to 12 hours and thus still systemically available to bind with the P2Y12 receptor after discontinuation of cangrelor infusion, allowing for these agents to be concomitantly administered without resulting in any DDI.5,6,11
Despite evidence indicating the lack of a DDI with the use of ticagrelor in cangrelor-treated patients, most data derive from studies in which ticagrelor was given at the time of initiation or during cangrelor infusion.5,6,11,12 To date, there are very limited data on the pharmacologic effects of cangrelor in patients pretreated with ticagrelor, and there are no studies that have been specifically designed to rule out a DDI when this occurs.13 This is of clinical relevance given that many patients in real-world clinical practice are pretreated with ticagrelor and in whom there may be a desire to use cangrelor to achieve enhanced P2Y12 inhibitory effects during PCI.14 This may include patients in whom the full antiplatelet effects of ticagrelor may be delayed by several hours due to impaired absorption such as in patients presenting with an acute coronary syndrome (ACS), particularly ST-segment elevation myocardial infarction (STEMI), or treated with opioids.15,16 The aim of this pharmacokinetic (PK) and pharmacodynamic (PD) study was to rule out a DDI associated with the use of cangrelor among patients pretreated with ticagrelor.
Methods
Study design and participants
The SWAP-5 (Switching Antiplatelet Therapy-5) study was a prospective, randomized, double-blind, placebo-controlled, crossover PK/PD investigation (NCT04634162). The study was performed at the University of Florida Health Science Center – Jacksonville. Patients were screened for eligibility during their regularly scheduled outpatient visits. Details on study inclusion and exclusion criteria are provided in the Supplemental Appendix. In brief, patients ≥18 years of age with stable coronary artery disease (CAD) on therapy with low-dose aspirin (81 mg daily) for at least 1 month were considered for enrollment. Key exclusion criteria included any active bleeding, high risk for bleeding, use of an oral P2Y12 receptor inhibitor or an oral anticoagulant in the prior 30 days, end-stage renal disease on hemodialysis, and known allergies to ticagrelor or cangrelor. The study complied with the Declaration of Helsinki and was approved by the Western Institutional Review Board, and all patients gave their written informed consent.
Using a computer-based randomization system, patients were randomly assigned in a 1:1 fashion to 1 of the following treatment arms: 1) ticagrelor loading dose (LD) followed after 1 hour by cangrelor bolus and infusion; or 2) ticagrelor LD followed after 1 hour by placebo bolus and infusion. Ticagrelor was administered as a 180-mg LD and cangrelor as a 30-μg/kg bolus followed by 4-μg/kg/min infusion. Cangrelor/placebo infusion was continued for a duration of 2 hours. After completing the first phase of the study, patients underwent a 1- to 4-week washout period and then crossed over to the alternative treatment in the second phase (ie, patients assigned to treatment with cangrelor in the first phase were assigned to placebo in the second phase and vice versa).
During each phase, PK and PD assessments were conducted at 7 time points (total 14 time points): baseline (prior to ticagrelor LD; time -1 hour); at start of cangrelor/placebo bolus and infusion (1 hour after ticagrelor LD; time 0); 30 minutes after cangrelor/placebo bolus; 1 hour after cangrelor/placebo bolus; 2 hours after cangrelor/placebo bolus (time of infusion discontinuation); 1 hour after discontinuation of cangrelor/placebo infusion; and 2 hours after discontinuation of cangrelor/placebo infusion. A period of 1 hour of pretreatment was chosen, as this approximates the time interval between drug administration and start of PCI in patients presenting with an STEMI, a setting in which cangrelor is most commonly used.16 Figure 1 illustrates the overall study design. The study had a double-blind design. Patients, research staff and laboratory personnel were blinded to treatment assignments. Masking and randomization of medications (cangrelor and placebo) were performed by our institutional research pharmacy in line with prior investigations.12
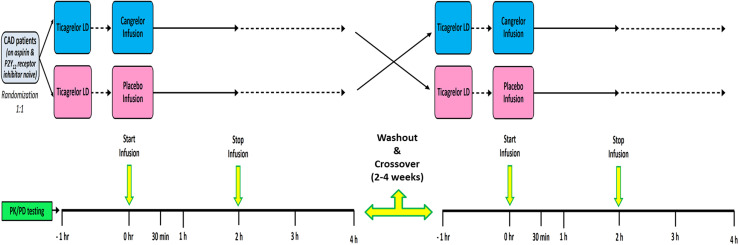
Figure 1. SWAP-5 Study Design
Study design diagram. CAD = coronary artery disease; LD = loading dose; PD = pharmacodynamic; PK = pharmacokinetic; SWAP-5 = Switching Antiplatelet Therapy-5.
During study treatment, major adverse cardiac events (death, myocardial infarction, stroke, and urgent revascularization procedures), serious adverse events (bleeding and other adverse events), and nonserious adverse events were collected. Ischemic adverse events were defined according to the Academic Research Consortium criteria, and bleeding was defined according to the Bleeding Academic Research Consortium definition.17,18
Blood sampling and laboratory assessments
A detailed description of PD and PK assessments is provided in the Supplemental Appendix. In brief, peripheral venous blood samples were drawn through a short venous catheter inserted into a forearm vein and collected in citrate, EDTA, and serum tubes as appropriate for assessments. The first 2 to 4 mL of blood were discarded to avoid spontaneous platelet activation. PD assessments were conducted using 4 different assays: 1) the VerifyNow PRU system (Werfen) with results reported in P2Y12 reaction units (PRU); 2) light transmittance aggregometry (LTA) (Chrono-Log Corp) following adenosine diphosphate (ADP) (20 μM) stimuli with results reported as maximum platelet aggregation; 3) whole blood vasodilator-stimulated phosphoprotein (VASP) (Biocytex Inc) with results reported as platelet reactivity index (PRI); and 4) the Total Thrombus-Formation Analysis System (T-TAS) (Diapharma) using a PL-chip with results reported as area under the curve (AUC).12,19, 20, 21, 22 PK assessments included determination of plasma concentration of ticagrelor and its major active metabolite (AR-C124910XX) as previously described (University of Vienna, Vienna, Austria).12 For ticagrelor and its active metabolite, the area under the plasma concentration vs time curve from time 0 to the last measurable concentration (AUC0-last), AUC from time 0 to 2 hours, maximum plasma concentration (Cmax), and time to Cmax were estimated.
Study endpoints and sample size calculation
The primary endpoint of the study was the noninferiority in PRU measured at 2 hours after discontinuation of cangrelor vs placebo. The primary hypothesis of our study was that in patients pretreated with a LD of ticagrelor followed by cangrelor infusion, platelet inhibition assessed by PRU would be noninferior to PRU in patients pretreated with a LD of ticagrelor LD followed by placebo infusion. Noninferiority was assessed using a 95% CI of the difference in mean PRU between the 2 arms. Under the assumption of zero difference in mean PRU between cangrelor and placebo and a common SD of 75 PRU, a sample size of 16 patients would allow for the 95% CI to stay within ±45 PRU with a 95% power and alpha = 0.05. Considering a 25% data attrition rate due to hemolysis, dropout, or technical problems, 20 patients needed to be randomized in order to ensure complete available data for analysis. Preliminary data and statistical assumptions for sample size calculation were established according to the results of previous PD investigations.12,15 In line with previously reported investigations, 45 PRU was chosen for the noninferiority margin for the upper 95% CI limit of the difference.20,23 All other endpoints were considered exploratory. These included the comparisons of PD and PK parameters and of rates of high on-treatment platelet reactivity (HPR). HPR was defined as PRU >208, PRI >50%, and LTA-ADP >59%, in line with consensus definitions.24, 25, 26
Statistical analysis
Categorical variables are expressed as frequencies and percentages and continuous variables as mean ± SD. Continuous variables were analyzed for normal distribution with the Kolmogorov-Smirnov test. Comparisons between categorical variables were performed using 2-tailed Fisher exact test or Pearson’s chi-square test. Student’s t-test was used to compare baseline continuous variables. For PD and PK data, treatment effects were evaluated comparing the functional parameters observed in the overall patient population after cangrelor treatment with those achieved after placebo regardless of the sequence. All statistical comparisons for the primary endpoint and exploratory endpoints with continuous variables were conducted using a linear mixed-effect model with treatment group, sequence, period, and treatment group by period as fixed effects and patient as a random effect. The comparisons of rates of HPR were conducted using the McNemar test.
Platelet reactivity results are reported as least-square mean (LSM) (95% CI) for the previously detailed analyses. LSM differences in PRU between groups and the corresponding 2-sided 95% CI for the difference were obtained to assess noninferiority based on the linear model. Given the exploratory nature of comparisons for secondary endpoints, correction for multiple comparisons was not performed. This is in line with previously reported investigations.15 A 2-tailed P value of <0.05 was considered to indicate a statistically significant difference for superiority for all the analyses performed. Statistical analysis was performed using SPSS version 28.0 software (IBM Corp). Graphs were plotted with GraphPad Prism version 9.1.0 (GraphPad Software).
The safety population included all randomized patients exposed to study medication. The PD population included all patients with PD data and without a major protocol deviation thought to affect the PD of cangrelor or ticagrelor significantly. The PD population was used for analysis of all primary and secondary PK/PD endpoints. The data, analytical methods, and study materials will not be made available to other researchers for purposes of reproducing the results or replicating the procedure.
Results
Patient population
Between February 17 and August 2, 2021, a total of 22 patients provided their written informed consent to participate in the study. Of these, 2 screen failed and 20 patients were randomized and received study medication, representing the safety population. All 20 patients completed phase 1 of the study (precrossover), also representing the PD population. One patient withdrew after phase 1, and 19 patients completed the second phase of the study (postcrossover) and have valid primary endpoint data. Patient characteristics are summarized in Table 1. There were no ischemic or major bleeding events during the course of the study. Ten patients experienced dyspnea: 2 in both the cangrelor and placebo phases, 2 in the placebo phase, and 6 in the cangrelor phase.
Table 1. Baseline Characteristics of the Pharmacodynamic Population (N = 20)
| Age, y | 68.4 ± 8.0 |
| Female | 11 (55.0) |
| Body mass index, kg/m2 | 34.2 ± 6.6 |
| Race | |
|---|---|
| Black | 10 (50.0) |
| White | 10 (50.0) |
| Current Smoking | 2 (10.0) |
| Hypertension | 20 (100.0) |
| Diabetes mellitus | 18 (90.0) |
| Hyperlipidemia | 17 (85.0) |
| Family history of premature CAD | 7 (35.0) |
| PAD | 1 (5.0) |
| Stroke | 2 (10.0) |
| Prior MI | 7 (35.0) |
| Prior PCI | 13 (65.0) |
| Prior CABG | 6 (30.0) |
| Congestive heart failure | 7 (35.0) |
| Left ventricular ejection fraction, % | 38.3 ± 15.1 |
| Medications | |
| ASA | 20 (100.0) |
| Statins | 19 (95.0) |
| Beta-blockers | 17 (85.0) |
| ACE inhibitors or ARBs | 14 (70.0) |
| Nitrates | 8 (40.0) |
| PPIs | 7 (35.0) |
| Calcium-channel blockers | 7 (35.0) |
| Oral antidiabetic drug | 10 (50.0) |
| Insulin | 8 (40.0) |
| Hemoglobin, g/dL | 13.2 ± 1.8 |
| Hematocrit, % | 40.0 ± 8.2 |
| Creatinine, mg/dL | 1.1 ± 0.3 |
| Platelet count, ×1,000/mm3 | 235.0 ± 62.1 |
Values are mean ± SD or n (%).
ACE = angiotensin-converting enzyme; ARB = angiotensin receptor blocker; ASA = acetylsalicylic acid; CABG = coronary artery bypass grafting; CAD = coronary artery disease; LVEF = left ventricular ejection fraction; MI = myocardial infarction; PAD = peripheral artery disease; PCI = percutaneous coronary intervention; PPI = proton pump inhibitor.
Pharmacodynamic findings
Platelet reactivity as assessed by VerifyNow PRU significantly decreased at 1 hour after ticagrelor LD. Adding cangrelor was associated with a significant reduction in PRU at 30 minutes (P = 0.001) and 1 hour (P = 0.005) after bolus administration as compared with placebo. No differences in PRU between treatments were observed at 1 and 2 hours after stopping infusion. At 2 hours after stopping cangrelor/placebo infusion (primary endpoint), PRU were similar between cangrelor and placebo (16.9 vs 12.6; LSM difference: 4.3; 95% CI: -28.6 to 37.3; P for superiority = 0.797), with the upper margin of the 95% CI of LSM difference below the 45 PRU noninferiority margin and meeting the primary noninferiority endpoint (Figure 2).
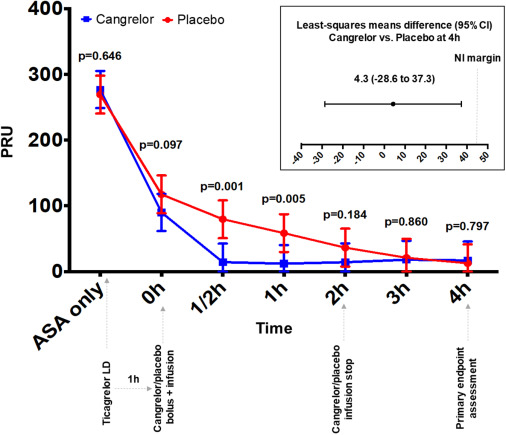
Figure 2. Pharmacodynamic Profile of Cangrelor vs Placebo Assessed by VerifyNow PRU
P2Y12 reaction units (PRU) measured by the VerifyNow P2Y12 assay. Values are expressed as least-squares means. Error bars indicate 95% CIs. P values indicate comparisons between groups at each time point. ASA = acetylsalicylic acid; LD = loading dose; NI = noninferiority.
Platelet reactivity assessed by LTA ADP, VASP, and T-TAS showed findings consistent with the VerifyNow PRU (Figure 3). In particular, maximum platelet aggregation and PRI were significantly lower with cangrelor vs placebo at 30 minutes and 1 hour after bolus with no differences at 2 hours after stopping infusion. AUC measured by T-TAS was lower in cangrelor-treated patients at 30 minutes, without any significant differences at the other time points.
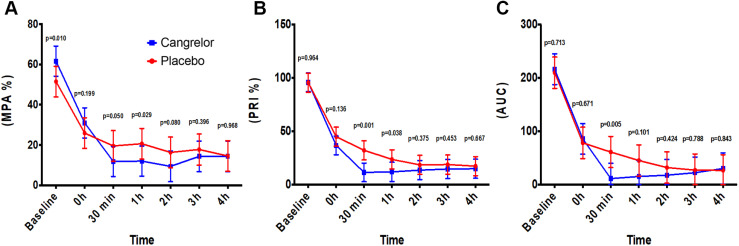
Figure 3. Pharmacodynamic Profiles of Cangrelor vs Placebo Assessed by Light Transmittance Aggregometry, Vasodilator-Stimulated Phosphoprotein, and Total Thrombus-Formation Analysis System
(A) Light transmittance aggregometry following adenosine diphosphate (20 μM) stimuli results reported as maximum platelet aggregation (MPA%). (B) Vasodilator-stimulated phosphoprotein results reported as platelet reactivity index (PRI%). (C) Total Thrombus-Formation Analysis System with results reported as the area under the curve (AUC). Values are expressed as least-squares means. Error bars indicate 95% CIs. P values indicate comparisons between groups at each time point.
HPR rates were reduced after ticagrelor LD administration and numerically lower in patients receiving cangrelor as compared with placebo without differences between groups after stopping cangrelor/placebo infusion (Supplemental Table 1).
Pharmacokinetic findings
PK profiles tracked PD findings. In particular, plasma levels of ticagrelor and its major active metabolite (AR-C124910XX) were similar between cangrelor and placebo at every time point (Figure 4). Overall, Cmax, AUC0-last, and AUC from time 0 to 2 hours for ticagrelor and AR-C124910XX were numerically increased in patients allocated to cangrelor compared with those allocated to placebo. Cangrelor was associated with a significant 44% increase in ticagrelor AUC0-last compared with placebo (5,025.8 [range: 1,998.0-8,846.8] ng·h/mL vs 3,487.7 [range: 247.4-8,599.7] ng·h/mL; P = 0.047). Time to Cmax was similar between cangrelor and placebo for both ticagrelor and AR-C124910XX (Table 2).
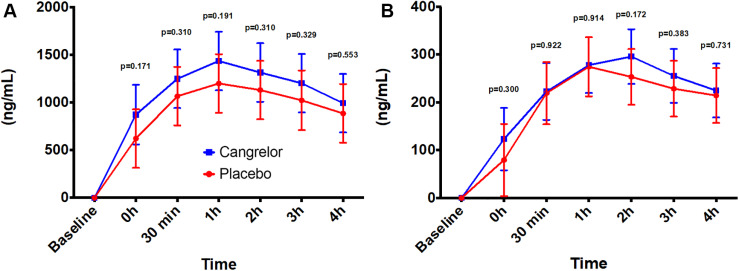
Figure 4. Plasma Concentrations of Ticagrelor and AR-C124910XX
Ticagrelor loading dose (180-mg orally) was administered at baseline 1 hour before the beginning of cangrelor bolus and infusion at time 0 hours. Plasma levels of (A) ticagrelor and (B) its major active metabolite AR-C124910XX during the 5 hours following the administration of ticagrelor loading dose. Values are expressed as means. Error bars indicate 95% CIs.
Table 2. Pharmacokinetic Profiles of Ticagrelor and AR-C124910XX
| Empty Cell | Cangrelor | Placebo | P Value |
|---|---|---|---|
| Ticagrelor | |||
| Tmax, h | 2.00 (1.00-5.00) | 2.00 (1.00-5.00) | 0.158 |
| Cmax, ng/mL | 1,695.3 (862.9-3,477.69) | 1,410.8 (195.8-2,866.9) | 0.259 |
| AUC0-2h, ng·h/mL | 2,429.0 (242.8-5,468.1) | 1,450.5 (63.4-5,141.5) | 0.156 |
| AUC0-last, ng·h/mL | 5,025.8 (1,998.0-8,846.8) | 3,487.7 (247.4-8,599.7) | 0.047 |
| AR-C124910XX | |||
| Tmax, h | 3.00 (1.50-5.00) | 3.00 (1.50-5.00) | 0.422 |
| Cmax, ng/mL | 312.3 (177.4-492.7) | 301.6 (124.1-701.8) | 0.731 |
| AUC0-2h, ng·h/mL | 443.0 (44.4-979.3) | 324.4 (44.5-1,078.5) | 0.274 |
| AUC0-last, ng·h/mL | 944.0 (214.3-1,762.7) | 815.4 (205.6-2,340.9) | 0.281 |
Tmax is reported as median (range). Cmax and AUC0-last are reported as geometric mean (range).
AUC0-last = AUC to the last measurable concentration; AUC0-2h = area under the curve from time 0 to 2 hours; Cmax = maximum observed plasma concentration; Tmax = time to maximum observed plasma concentration.
Discussion
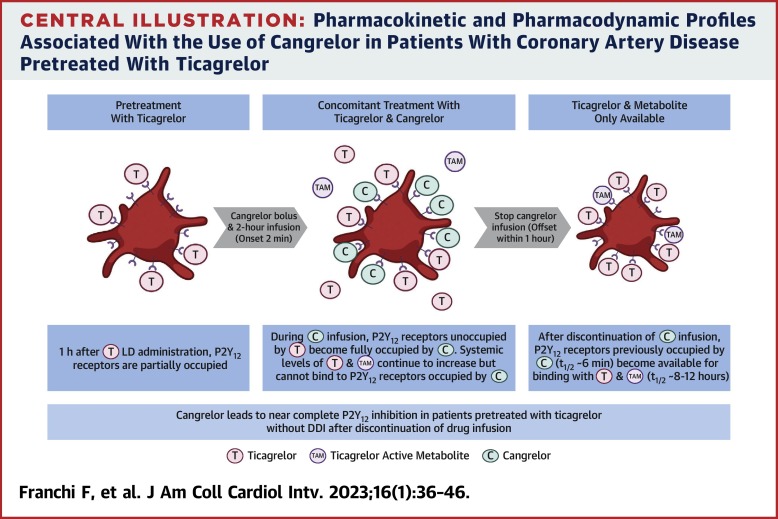
The SWAP-5 study is the first study specifically designed to rule out a DDI in cangrelor-treated patients who have been pretreated with ticagrelor. In particular, we chose a randomized, double-blind, placebo-controlled, crossover investigation with carefully selected time points to perform PK and PD assessments to test our study hypothesis. Moreover, multiple PD assays were used to corroborate our study findings. The key observations from our study were that, among patients who have been pretreated 1-hour prior with a 180-mg LD of ticagrelor: 1) compared with placebo, cangrelor further enhances P2Y12 inhibitory effects up to 1 hour after initiation of bolus and infusion; 2) platelet reactivity among cangrelor-treated patients was noninferior to that observed among placebo-treated patients at 2 hours after discontinuation of drug infusion, ruling out a DDI; and 3) PK analysis showed that, compared with placebo, cangrelor was associated with numerically increased exposure to ticagrelor and its active metabolite. Overall, these observations show that even with ticagrelor pretreatment, the use of cangrelor can blunt the initial gap in platelet inhibition observed with the use of a potent oral P2Y12 inhibitor (ie, ticagrelor) without concerns of a DDI (Central Illustration).
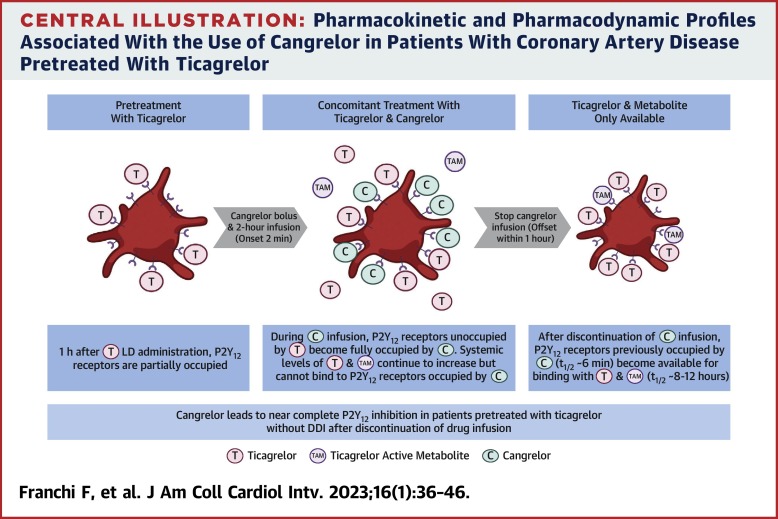
Central Illustration. Pharmacokinetic and Pharmacodynamic Profiles Associated With the Use of Cangrelor in Patients With Coronary Artery Disease Pretreated With Ticagrelor
The ticagrelor active metabolite is AR-C124910XX. DDI = drug-drug interaction; LD = loading dose; t1/2 = half-life.
Cangrelor is a nonthienopyridine analog of adenosine triphosphate with reversible inhibitory effects on the platelet P2Y12 receptor.7 Cangrelor is administered intravenously, and following bolus administration (30 μg/kg), it reaches its maximum concentration in 2 minutes, leading to profound platelet P2Y12 inhibition.7 Because of its very short half-life (3-6 minutes), cangrelor has a fast offset of action, and restoration of normal platelet function occurs within 60 minutes following discontinuation of infusion.7 Because of its prompt and potent antiplatelet effects, cangrelor was developed to mitigate the risk of periprocedural thrombotic complications in patients undergoing PCI who have not been pretreated with an oral P2Y12 inhibitor.1 Indeed, its rapid offset of action allows cangrelor to exert its effects when most needed (ie, during the PCI procedure), minimizing the risk of bleeding complications commonly associated with other potent antiplatelet therapies, such as glycoprotein IIb/IIIa inhibitors, that have a longer offset of action.27 However, because cangrelor shares the same target on the platelet membrane surface as the oral P2Y12 inhibitors, the clinical development of cangrelor for PCI had to take into consideration the potential for a DDI that would inevitably mitigate or even abolish any platelet inhibitory effect of an oral agent (ie, clopidogrel) if given concomitantly with cangrelor, resulting in lack of antithrombotic protection following discontinuation of cangrelor infusion.5, 6, 7, 8, 9, 10 Indeed, a critical aspect of the clinical trial development of cangrelor was the need for judicious transitioning from intravenous to oral treatment. Accordingly, all phase 3 clinical trials of cangrelor in PCI entailed the administration of clopidogrel, the oral P2Y12 inhibitor of choice at the time of trials design, at the end of cangrelor infusion to avoid such DDI.1,28,29
The broader uptake of the newer-generation oral P2Y12 inhibitors prasugrel and ticagrelor by the end of the clinical trial programs of cangrelor enhanced interest in how to use these agents among cangrelor treated patients.30 Similar to clopidogrel, prasugrel is a thienopyridine that requires metabolic activation to generate an active metabolite. Because the active metabolites of thienopyridines (clopidogrel and prasugrel) have half-lives that do not exceed the duration of the recommended infusion of cangrelor, generally 2 to 4 hours, they are mostly cleared from systemic circulation by the time the P2Y12 receptors become available for binding following discontinuation of cangrelor infusion.5,6 Accordingly, it is recommended that clopidogrel and prasugrel be administered at the end of the cangrelor infusion to avoid a DDI.2,6 Because ticagrelor has a half-life of 6 to 12 hours, it is still systemically available to bind with the P2Y12 receptor after discontinuation of cangrelor infusion.2,6 Accordingly, ticagrelor and cangrelor can be concomitantly administered without resulting in any DDI. Because cangrelor is more commonly used in patients presenting with an ACS, and the newer-generation P2Y12 inhibitors are preferred over clopidogrel in this setting, ticagrelor is the most commonly used oral P2Y12 inhibitor in real-world practice of patients treated with cangrelor.14,31
Cangrelor was developed for patients undergoing PCI who have not been pretreated with an oral P2Y12 inhibitor.1 Despite guidelines no longer advocating for routine upstream use of an oral P2Y12 inhibitor, many ACS patients are still treated at time of clinical presentation.3,4 This is particularly true for ticagrelor, given that in the phase 3 clinical trial leading to its approval, ticagrelor was administered at time of diagnosis of an ACS, irrespective of management (invasive or noninvasive) and prior to defining coronary anatomy.32 In our study, we were able to show that cangrelor was able to exert additional P2Y12 inhibitory effects in patients who had already been treated with ticagrelor. These findings are in line with in vitro findings previously reported from our group and can be attributed to the fact that cangrelor is associated with very high P2Y12 receptor occupancy and can thus inhibit receptors that have not been occupied by an oral agent.33 Indeed, it may be argued that in our study patients were pretreated with ticagrelor for only 1 hour prior to the start of cangrelor infusion, hence not allowing sufficient time for it to achieve its full antiplatelet effects, which requires at least 2 hours in a stable setting, as also demonstrated in our investigation.34 However, it is not uncommon for many patients presenting with an ACS, particularly those with STEMI, to have such a short, or even shorter, time frame of pretreatment.35,36 Particularly, in STEMI patients in whom oral drug absorption is delayed due the hemodynamic conditions associated with this clinical condition, as well as the frequent use of opioid products also associated with impaired absorption, the full effects of an oral P2Y12 inhibitor may take up to 6 hours.15,16
The lack of efficacy associated with upstream treatment of a potent oral P2Y12 inhibitor, even if administered in crushed formulation, in patients with STEMI undergoing primary PCI with short time frames (ie, up to 1 hour) underscores the need to bridge the gap in platelet inhibition in these patients.12,35,36 Such observations underscore the clinical implications of our PK/PD investigation. Indeed, although our study was not conducted in a cohort of patients in whom oral drug absorption is impaired, it still showed that cangrelor is able to bridge the gap in platelet inhibition until the full effects of an oral drug is achieved. The magnitude of such effect would inevitably be larger in an acute setting, as previously shown in another PD investigation from our group in which ticagrelor, administered in a crushed formulation, was given at the start of PCI.12 Most importantly, the key finding of our study, in line with the hypothesis of our investigation, is that cangrelor can be used even if patients have been pretreated with ticagrelor without resulting in a DDI as demonstrated by the absence of differences in PD findings, measured according to statistical principles of noninferiority, at 2 hours following discontinuation of cangrelor/placebo infusion, when ticagrelor achieved profound P2Y12 inhibitory effects in both treatment arms. Indeed, it may be argued that the oral P2Y12 inhibitor used among cangrelor-treated patients may impact the degree of platelet inhibition observed. In fact, a recently reported PD investigation that showed that cangrelor provided inferior platelet inhibition compared with tirofiban, prasugrel was the oral P2Y12 inhibitor used and administered at the end of cangrelor infusion.26 However, platelet inhibition at 3 to 4 hours was still lower with cangrelor even when prasugrel was chewed. The reasons for the diverse PD profiles observed among studies can be related to the different pharmacologic profiles of prasugrel and ticagrelor. In our study, only 1 patient was found to have HPR at 30 minutes of cangrelor infusion according to VerifyNow and at 1 hour according to LTA and VASP; adequate platelet inhibition was observed at subsequent time points. Overall, these observations indicate that HPR during cangrelor infusion is very rare and, importantly, that the use of ticagrelor as oral P2Y12 inhibitor, instead of thienopyridines, particularly clopidogrel, allows for a transition that mitigates gaps in platelet inhibition as also confirmed in other observational PD investigations.37
In addition, exposure to ticagrelor and its major metabolite were numerically higher in patients receiving cangrelor. Although the mechanism leading to increased AUC and Cmax is unknown, it may be speculated that the very high level of P2Y12 receptor occupancy by cangrelor would result in more unbound ticagrelor and AR-C124910XX in the plasma during cangrelor infusion vs placebo. Because of the nearly identical speed of absorption and plasma levels at 2 hours after stopping the infusion, the clinical implications of higher exposure to ticagrelor is likely marginal. Overall, the PK/PD findings of our study open future avenues for clinical investigation with cangrelor among high-risk patients pretreated with ticagrelor.
Study limitations
The PK/PD nature of this investigation does not allow to draw any conclusions on the safety or efficacy on the use of cangrelor among patients pretreated with ticagrelor. The ongoing CAMEO (Cangrelor in Acute Myocardial Infarction: Effectiveness and Outcomes) registry (NCT04076813) as well as other registries will provide insights on clinical outcomes associated with the use of cangrelor in real-world clinical practice, including those pretreated with ticagrelor, which, however, to date have not raised any safety or efficacy concerns.14,38 Further, our study was conducted in patients with stable CAD and not in patients with ACS undergoing PCI. Hence, the magnitude of the PK/PD findings observed in our study may not be reflective of those in the acute setting. Nevertheless, the placebo-controlled nature of our study conducted with a crossover design with measures of both PK and PD is the most rigorous form to conduct a study to rule out a DDI and would have not been feasible in an acute setting. Finally, in our study, pretreatment occurred only 1 hour before starting cangrelor, and cangrelor infusion was maintained for 2 hours. Thus, the PK/PD effects associated with longer time frames of pretreatment and infusion duration cannot be deducted from our investigation.
Conclusions
In patients with stable CAD who have been pretreated with ticagrelor, the use of cangrelor was associated with no significant differences in PK/PD profiles after discontinuation of drug infusion indicating the absence of a DDI. In addition, in such patients cangrelor led to enhanced P2Y12 inhibition allowing to bridge the gap in platelet inhibitory effects associated with oral therapies. Future studies conducted in patients with ACS undergoing PCI are warranted to define the clinical implications of such pharmacologic treatment regimen.
Funding Support and Author Disclosures
The present study was funded by an investigator-initiated grant from The Scott R. MacKenzie Foundation. The Scott R. MacKenzie Foundation had no role in the study design conception, conduct of the study, or decision to publish these results. Dr Franchi has received consulting fees or honoraria from AstraZeneca, Bayer, and Sanofi; and has received institutional payments for grants from PLx Pharma and The Scott R. MacKenzie Foundation. Dr Angiolillo has received consulting fees or honoraria from Abbott, Amgen, AstraZeneca, Bayer, Biosensors, Boehringer Ingelheim, Bristol Myers Squibb, Chiesi, Daiichi Sankyo, Eli Lilly, Haemonetics, Janssen, Merck, Novartis, PhaseBio, PLx Pharma, Pfizer, and Sanofi; and has received research grants to the institution from Amgen, AstraZeneca, Bayer, Biosensors, CeloNova, CSL Behring, Daiichi Sankyo, Eisai, Eli Lilly, Gilead, Idorsia, Janssen, Matsutani Chemical Industry Co, Merck, Novartis, and The Scott R. MacKenzie Foundation. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
References
- D.L. Bhatt, G.W. Stone, K.W. Mahaffey, et al.Effect of platelet inhibition with cangrelor during PCI on ischemic eventsN Engl J Med, 368 (2013), pp. 1303-1313 View at publisher CrossRef View in Scopus Google Scholar
- D.J. Angiolillo, M. Galli, J.P. Collet, A. Kastrati, M.L. O’DonoghueAntiplatelet therapy after percutaneous coronary interventionEuroIntervention, 17 (2022), pp. e1371-e1396 View at publisher CrossRef Google Scholar
- J.S. Lawton, J.E. Tamis-Holland, S. Bangalore, et al.2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice GuidelinesJ Am Coll Cardiol, 79 (2) (2022), pp. e21-e129 View PDF View article View in Scopus Google Scholar
- J.P. Collet, H. Thiele, E. Barbato, et al.2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevationEur Heart J, 42 (2021), pp. 1289-1367 View at publisher This article is free to access.CrossRef View in Scopus Google Scholar
- D.J. Angiolillo, F. Rollini, R.F. Storey, et al.International expert consensus on switching Platelet P2Y12 receptor-inhibiting therapiesCirculation, 136 (2017), pp. 1955-1975View in Scopus Google Scholar
- F. Rollini, F. Franchi, D.J. AngiolilloSwitching P2Y12-receptor inhibitors in patients with coronary artery diseaseNat Rev Cardiol, 13 (2016), pp. 11-27 View at publisher CrossRef View in Scopus Google Scholar
- D.J. Angiolillo, D.J. Schneider, D.L. Bhatt, et al.Pharmacodynamic effects of cangrelor and clopidogrel: the platelet function substudy from the cangrelor versus standard therapy to achieve optimal management of platelet inhibition (CHAMPION) trialsJ Thromb Thrombolysis, 34 (2012), pp. 44-55 View at publisher CrossRef View in Scopus Google Scholar
- S.R. Steinhubl, J.J. Oh, J.H. Oestreich, S. Ferraris, R. Charnigo, W.S. AkersTransitioning patients from cangrelor to clopidogrel: pharmacodynamic evidence of a competitive effectThromb Res, 121 (2008), pp. 527-534 View PDF View article View in Scopus Google Scholar
- D.J. Schneider, Z. Agarwal, N. Seecheran, P. GogoPharmacodynamic effects when clopidogrel is given before cangrelor discontinuationJ Interv Cardiol, 28 (2015), pp. 415-419 Google Scholar
- D.J. Schneider, N. Seecheran, S.S. Raza, F.K. Keating, P. GogoPharmacodynamic effects during the transition between cangrelor and prasugrelCoron Artery Dis, 26 (2015), pp. 42-48 View in Scopus Google Scholar
- D.J. Schneider, Z. Agarwal, N. Seecheran, F.K. Keating, P. GogoPharmacodynamic effects during the transition between cangrelor and ticagrelorJ Am Coll Cardiol Intv, 7 (2014), pp. 435-442 View PDF View article View in Scopus Google Scholar
- F. Franchi, F. Rollini, A. Rivas, et al.Platelet inhibition with cangrelor and crushed ticagrelor in patients with ST-segment-elevation myocardial infarction undergoing primary percutaneous coronary interventionCirculation, 139 (2019), pp. 1661-1670 View at publisher CrossRef View in Scopus Google Scholar
- M.A. Mohammad, P. Andell, S. Koul, et al.Cangrelor in combination with ticagrelor provides consistent and potent P2Y12-inhibition during and after primary percutaneous coronary intervention in real-world patients with ST-segment-elevation myocardial infarctionPlatelets, 28 (2017), pp. 414-416 View at publisher CrossRef View in Scopus Google Scholar
- P. Grimfjard, B. Lagerqvist, D. Erlinge, C. Varenhorst, S. JamesClinical use of cangrelor: nationwide experience from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR)Eur Heart J Cardiovasc Pharmacother, 5 (2019), pp. 151-157 View at publisher This article is free to access. CrossRef View in Scopus Google Scholar
- F. Franchi, F. Rollini, Y. Park, et al.Effects of methylnaltrexone on ticagrelor-induced antiplatelet effects in coronary artery disease patients treated with morphineJ Am Coll Cardiol Intv, 12 (2019), pp. 1538-1549 View PDF View article View in Scopus Google Scholar
- F. Franchi, F. Rollini, D.J. AngiolilloAntithrombotic therapy for patients with STEMI undergoing primary PCINat Rev Cardiol, 14 (2017), pp. 361-379 View at publisher CrossRef View in Scopus Google Scholar
- R. Mehran, S.V. Rao, D.L. Bhatt, et al.Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research ConsortiumCirculation, 123 (2011), pp. 2736-2747 View in Scopus Google Scholar
- H.M. Garcia-Garcia, E.P. McFadden, A. Farb, et al.Standardized end point definitions for coronary intervention trials: the Academic Research Consortium-2 consensus documentCirculation, 137 (2018), pp. 2635-2650 View at publisher CrossRef View in Scopus Google Scholar
- D.J. Angiolillo, J.J. Badimon, J.F. Saucedo, et al.A pharmacodynamic comparison of prasugrel vs. high-dose clopidogrel in patients with type 2 diabetes mellitus and coronary artery disease: results of the Optimizing anti-Platelet Therapy In diabetes MellitUS (OPTIMUS)-3 TrialEur Heart J, 32 (2011), pp. 838-846 View at publisher This article is free to access. CrossRef View in Scopus Google Scholar
- D.J. Angiolillo, N. Curzen, P. Gurbel, et al.Pharmacodynamic evaluation of switching from ticagrelor to prasugrel in patients with stable coronary artery disease: Results of the SWAP-2 Study (Switching Anti Platelet-2)J Am Coll Cardiol, 63 (2014), pp. 1500-1509 View PDF View article View in Scopus Google Scholar
- F. Franchi, G.T. Faz, F. Rollini, et al.Pharmacodynamic effects of switching from prasugrel to ticagrelor: results of the prospective, randomized SWAP-3 studyJ Am Coll Cardiol Intv, 9 (2016), pp. 1089-1098 View PDF View article View in Scopus Google Scholar
- S. Kikuchi, K. Tsukahara, S. Ichikawa, et al.Platelet-derived thrombogenicity measured by total thrombus-formation analysis system in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary interventionCirc J, 84 (2020), pp. 975-984 View at publisher CrossRef View in Scopus Google Scholar
- F. Franchi, F. Rollini, J. Rivas Rios, et al.Pharmacodynamic effects of switching from ticagrelor to clopidogrel in patients with coronary artery disease: results of the SWAP-4 studyCirculation, 137 (2018), pp. 2450-2462 View at publisher CrossRef View in Scopus Google Scholar
- D. Sibbing, D. Aradi, D. Alexopoulos, et al.Updated expert consensus statement on platelet function and genetic testing for guiding P2Y12 receptor inhibitor treatment in percutaneous coronary intervention J Am Coll Cardiol Intv, 12 (2019), pp. 1521-1537 View PDF View article View in Scopus Google Scholar
- L. Bonello, U.S. Tantry, R. Marcucci, et al.Consensus and future directions on the definition of high on-treatment platelet reactivity to adenosine diphosphateJ Am Coll Cardiol, 56 (2010), pp. 919-933 View PDF View article View in Scopus Google Scholar
- G. Gargiulo, G. Esposito, P. Cirillo, et al.Facilitation Through Aggrastat or Cangrelor Bolus and Infusion Over PrasugreL: a MUlticenter Randomized Open-label Trial in PatientS with ST-elevation Myocardial InFarction Referred for PrimAry PercutaneouS InTERvention (FABOLUS FASTER) trial: design and rationaleJ Cardiovasc Transl Res, 14 (2021), pp. 110-119 View at publisher CrossRef View in Scopus Google Scholar
- D. Capodanno, R.P. Milluzzo, D.J. AngiolilloIntravenous antiplatelet therapies (glycoprotein IIb/IIIa receptor inhibitors and cangrelor) in percutaneous coronary intervention: from pharmacology to indications for clinical use Ther Adv Cardiovasc Dis, 13 (2019), Article 1753944719893274 View at publisher This article is free to access.View in Scopus Google Scholar
- D.L. Bhatt, A.M. Lincoff, C.M. Gibson, et al.Intravenous platelet blockade with cangrelor during PCIN Engl J Med, 361 (2009), pp. 2330-2341 View at publisher CrossRef View in Scopus Google Scholar
- R.A. Harrington, G.W. Stone, S. McNulty, et al.Platelet inhibition with cangrelor in patients undergoing PCIN Engl J Med, 361 (2009), pp. 2318-2329 View at publisher CrossRef View in Scopus Google Scholar
- F. Franchi, D.J. AngiolilloNovel antiplatelet agents in acute coronary syndromeNat Rev Cardiol, 12 (2015), pp. 30-47View at publisher CrossRef View in Scopus Google Scholar
- J.A. Rymer, D.L. Bhatt, D.J. Angiolillo, et al.Cangrelor use patterns and transition to oral P2Y12 inhibitors among patients with myocardial infarction: initial results from the CAMEO registryJ Am Heart Assoc, 11 (2022), Article e024513 View in Scopus Google Scholar
- L. Wallentin, R.C. Becker, A. Budaj, et al.Ticagrelor versus clopidogrel in patients with acute coronary syndromesN Engl J Med, 361 (2009), pp. 1045-1057 View at publisher CrossRef View in Scopus Google Scholar
- F. Rollini, F. Franchi, E. Thano, et al.In vitro pharmacodynamic effects of cangrelor on platelet P2Y12 receptor-mediated signaling in ticagrelor-treated patientsJ Am Coll Cardiol Intv, 10 (2017), pp. 1374-1375 View PDF View article View in Scopus Google Scholar
- S. Husted, H. Emanuelsson, S. Heptinstall, P.M. Sandset, M. Wickens, G. PetersPharmacodynamics, pharmacokinetics, and safety of the oral reversible P2Y12 antagonist AZD6140 with aspirin in patients with atherosclerosis: a double-blind comparison to clopidogrel with aspirinEur Heart J, 27 (2006), pp. 1038-1047 View at publisher This article is free to access. CrossRef View in Scopus Google Scholar
- G. Montalescot, A.W. van ‘t Hof, F. Lapostolle, et al.Prehospital ticagrelor in ST-segment elevation myocardial infarctionN Engl J Med, 371 (2014), pp. 1016-1027 View at publisher CrossRef View in Scopus Google Scholar
- G.J. Vlachojannis, J.M. Wilschut, R.F. Vogel, et al.Effect of prehospital crushed prasugrel tablets in patients with ST-segment-elevation myocardial infarction planned for primary percutaneous coronary intervention: the randomized COMPARE CRUSH trial Circulation, 142 (2020), pp. 2316-2328 View at publisher CrossRef View in Scopus Google Scholar
- G. Gargiulo, A. Marenna, L. Sperandeo, et al.Pharmacodynamic effects of cangrelor in elective complex PCI: insights from the POMPEII study EuroIntervention (Published online December 13, 2022), 10.4244/EIJ-D-22-594 View at publisher Google Scholar
- L. De Luca, P.G. Steg, D.L. Bhatt, D. Capodanno, D.J. AngiolilloCangrelor: clinical data, contemporary use, and future perspectives J Am Heart Assoc, 10 (2021), Article e022125 View in Scopus Google Scholar